
Vista
Bronze
- Joined
- Mar 6, 2020
- Posts
- 359
- Reputation
- 394
- OP
- #101
to optimise natural gh release during sleepWhy should we avoid eating 3 hours before bedtime?
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: this_feature_currently_requires_accessing_site_using_safari
to optimise natural gh release during sleepWhy should we avoid eating 3 hours before bedtime?
its pretty much random, usually your face will grow (as does everything else, like height) when you take GH so your face growth should be "proportional" to your height gains, but since your plates are almost definitely fused you might experience less vertical growth and instead some frame growth (if your clavicle plates are still open).Very good thread bro.
I was thinking about administering IGF1 or mk677 at almost 23 years old to try at least gain 1 or 2cm in height to go from 6'1.5 to 6'2.5 (at night) and maybe add frame
I see about a guy here on the forum who grew a few inches at 23 after taking GH and some other things, so that gave me some hope.
but I'm a little afraid of affecting my facial proportions (which are considerably good). Do you have any idea of the incidence of minimal changes to the face?
Great thread but doesn't beat the current one in BOTB. You'll get a lot of redirects though from that thread.
Introduction
As many of you know ‘heightmaxing’ is a popular topic of discussion on this website, which is no surprise given the importance of height on attractiveness as well as a plethora of other benefits associated with being taller.
I’m sure we’re all familiar with the importance of height, but there is a concerning deficit of information regarding methods and knowledge on how to engender an increase of height.
This shouldn’t come as much of a surprise, since the mechanisms behind increasing your height are very complex and we still don’t know a lot about the subject. Many factors work together to determine height and there is a lot of disagreement in the scientific community on the subject.
The purpose of this guide is to take a relatively simplistic, scientific and easy to understand approach to height maxing, which will hopefully dispel some of the confusion on the subject. The ‘science’ bits will be written in red for those wanting elaboration.
View attachment 2423234
Overview of the mechanisms involved in growing taller
1) Activation Phase: This is the beginning of bone growth. Cells called chondrocytes (cartilage) come together and proliferate (replicate). They create a blueprint made of cartilage, like a model for the bone to follow.
2) Osteoclast Recruitment and Resorption Phase (Hypertrophy Phase): Chondrocytes grow bigger (hypertrophy) and start turning the cartilage into hard stuff. Think of them as builders laying down the foundation for the bone.
3) Reversal Phase (Osteoblast Phase): A group of cells called osteoblasts moves in. They see the blueprint created by the cartilage and start adding bone on stop.
4) Formation Phase (Calcification Phase): The material the osteoblasts add becomes hard and strong because it calcifies, which is like turning it into concrete. Picture the bone getting denser and stronger.
5) Mineralization Phase (Ossification Phase): This is when the bone really takes shape. More bone cells come in, and they keep building and strengthening the bone, kind of like construction workers finishing a house.
6) Closure Phase (Epiphyseal Plate Closure): During adolescence, special plates at the ends of your long bones, called epiphyseal plates or growth plates, are active and contribute to your height. But once you reach a certain age, usually 15- 17, these plates close up.
View attachment 2423236
During osteoclastogenesis phases 1- 5 are constantly repeating in a loop until the closure phase.
The phase in osteoclastogenesis (bone growth) which contributes to enlarging your longitudinal height the most is the activation phase, which starts when you are an embryo and ends with the closure phase.
Now the question becomes: how do I enhance the mechanisms of the activation phase.
During the activation phase cartilage grows through proliferation and differentiation.
Cell proliferation = Cell gets bigger + Cell divides, AKA More cells
View attachment 2423237
For the purpose of heightmaxing, proliferation is one of the important mechanisms that drives height growth.There are some things we can do to increase the proliferation and hypertrophy of cartilage in the growth plate. This is done through bone growth factors, which work through a variety of different mechanisms and pathways.
We need to do everything possible to enhance cell proliferation and cell size in the growth plate.
What we need to do to heightmax
1) Increase cartilage proliferation (replication)
2) Increase cartilage hypertrophy (size)
3) Delay the closure phase
One of the ways we can increase proliferation and hypertrophy is with growth factors (a subset of cytokines).
An Introduction To Growth Factors & Hormones
Known bone growth factors (outside of foetal development) include:
- Insulin-like growth factor-1 (IGF-1) is the most abundant growth factor deposited in the bone matrix and stimulates cell proliferation and function, and survival of osteoblasts.
- There are several reports demonstrating the synergistic effects of IGF-1 and PTH on bone remodelling and establishing the involvement of locally produced IGF-1 in the anabolic effects of PTH
- PTH can exert both catabolic and anabolic effects on bone. It is well established that daily injections of low doses of PTH increase bone mass in animals and humans
- Transforming growth factor beta (TGF-β)
- TGF-β1
- TGF-β3
- Sort of a double edged sword, can cause an increase of bone mass but also osteoporosis, it is best to use this as little as possible.
- Fibroblast growth factors (FGF)
- FGF 1 - 10
- FGF18
- Endogenous FGF-2 was found to be necessary for the bone anabolic effects of PTH and BMP-2 in mice
- Platetet- Derived Growth Factor (PDGF)
- Growth Differentiation Factor (GDF)
- GDF3
- GDF6
- GDF10
- Fibroblast Growth Factor (FGF)
Hormones also play a role in height and morphology, a brief overview of which is provided below:
- Growth Hormone:
- Stimulates IGF-1 growth factor AND IGF-1 receptor production. Growth hormone (GH) is a peptide hormone secreted from the pituitary gland under the control of the hypothalamus. It has been reported that both GH-deficient humans and mice have reduced longitudinal bone growth
- Testosterone & DHT:
- Broadens Shoulders & promotes sexual dimorphism. Androgens can also modulate growth plate maturation and closure, and thus affect longitudinal bone growth. In addition, androgens regulate trabecular and cortical bone mass, and inhibit bone loss
- Oestrogen (Estrogen):
- Causes the hips to widen and become rounded & speed up the rate of Growth Plate fusion (more on this in part 4). Oestrogen is also needed for healthy bones.
- Thyroid Hormones: Thyroid hormones, particularly thyroxine (T4) and triiodothyronine (T3) promote chondrocyte proliferation and the synthesis of collagen and other bone matrix proteins.
Something rarely mentioned in heightmaxing is Growth Factor receptors, growth factor receptors and growth factors as two puzzle pieces, they need each other to work.
There aren’t many ways to directly increase Growth factor receptors, but some studies suggest that increasing one growth factor can signal others to proliferate.
What this also means is that depending on your specific distribution of growth factor receptors your growth will be somewhat random. People who have more receptors in their legs/ epiphyseal plate will experience more growth in that area than someone with more receptors in their shoulders or nose.
View attachment 2423238
Primary Growth Factors - Factors that lead to the most growth
An overview of some of the process' involved promoting bone growth
Applying Growth Factors
IGF-1 (IGF-1 LR3)
One of the most popular growth factors on looksmax for heightmaxing is IGF-1, which granted its price and efficacy should come as no surprise . Another advantage of IGF-1 is that it binds and activates its own receptor.Among the insulin-like growth factor 1 (IGF-1) analogues, the one with the best balance between potency and half life is IGF-1 LR3. It has a half life of between 20-30 hours and a stronger binding affinity than naturally occurring IGF-1
Growth Hormone (HGH)
Again, a very popular growth factor on this website. Growth hormone (GH) is a peptide hormone secreted from the pituitary gland under the control of the hypothalamus. GH, along with its binding protein (GHBP), regulates growth directly through the GH receptor (GHR) and indirectly by stimulating liver and skeletal IGF-1 expression.It has been reported that GH stimulates osteoblast proliferation and collagen production either directly and/or indirectly by increasing IGF-1 and IGF binding protein (IGFBP) productionThese effects make GH useful, mostly due to its signalling properties and ability to upregulate the number of Growth Hormone receptors. While the increase in IGF-1 is also useful, we already know that synthetic IGF-1 analogues like IGF-1 LR3 are more potent, meaning that both GH and IGF-1 LR3 could be used synergistically. PTH
A compound not typically discussed on this forum is Parathyroid hormone.Parathyroid hormone (PTH), also called parathormone or parathyrin, is a peptide hormone secreted by the parathyroid glands.As mentioned earlier, PTH and IGF-1 are known to have synergistic effects, therefore it is advantageous to be running both IGF and PTH in the same stack.
View attachment 2423240
Osteogenic differentiation of BMSCs treated with vehicle (-), IGF-1 (50 ng·mL-1), PTH (100 nmol·L-1), or both as assessed by alkaline phosphatase.
We can see that using both IGF and PTF gives us significantly more growth.
Secondary Growth Factors - Factors That Support Growth
Calcitriol
Calcitriol is the biologically active form of vitamin D in the body. It is also known as 1,25-dihydroxyvitamin D3 or simply activated vitamin D. It is up to 1,000 times more potent than vitamin d2 and d3, making it ideal for supporting growth.
Testosterone & DHT
By far one of the most influential androgens on height and the development of a sexually dimorphic skeleton. The androgen mechanism of action on height is not well understood, but it is known to stimulate longitudinal bone growth as well as radial bone growth, thereby increasing the cortical bone size.
Lifestyle/ Diet
By far one of the most under looked growth factors is your lifestyle, it is often the easiest and one of the most impactful on your height.Eating enough food is vital to create the building blocks of hormones/ growth factors, ultimately increasing your height. It has been suggested that in addition to adequate intake of macro and micronutrients (vitamins, minerals, amino acids) intermittent fasting can also be beneficial for raising IGF-1 and increasing insulin sensitivity. Diets high in protein and dairy (not including cheese) were also found to elevate IGF-1.Adequate sleep, minimal stress and regular exercise are also seen to have positive effects on height.Delaying Growth Plate Fusion“Oestrogen causes maturation of the growth plate, accelerating skeletal maturation and the accumulation of minerals into the cartilage. Oestrogen also promotes the closure of the physis, stopping the axial growth of the bone. Decreases in total oestrogen or oestrogen receptor sensitivity results in longer bones and tall stature”What this means is that oestrogen is one of the driving forces behind signalling the closure phase. One of the ways Oestrogen can be regulated is via a class of drugs called antioestrogens.
Antioestrogens I recommend:
- Exemestane (Aromasin) is relatively easy to get, has a long half life (24 hours), low side effects and decent bioavailability.
- Letrozole has also been shown to delay the fusing of the growth plates in mice. When used in combination with growth hormone, letrozole has been shown effective in one adolescent boy with a short stature. Mice administered with Letrozole were also found to have higher testosterone levels. I recomend cycling Lerozole with Aromasin.
Growing Taller
If you are 15 and over I recommend getting an x- ray done of your epiphyseal plate to confirm whether or not it has fused. Complete fusion of the growth plate most commonly occurs between 15-17 in males (and no, you’re probably not an exception).
If your epiphyseal plate is open great, if not then you can still apply some of these methods to improve your frame. All bones fuse at different times, so even though your epiphyseal plate is sealed your other bones, such as the tibia and collarbone may still be open, allowing you to grow (more on this below).
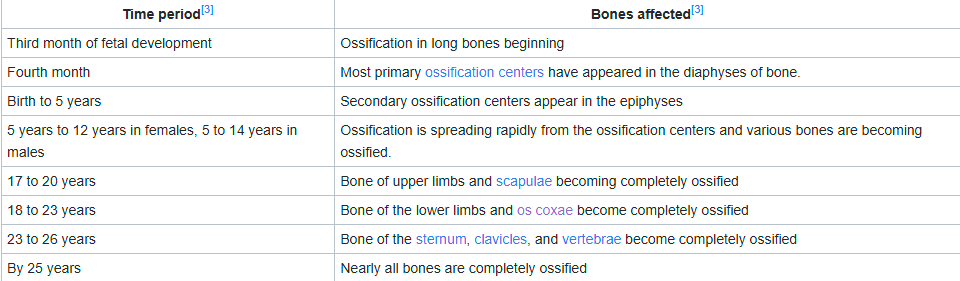
It is also worth noting that Europeans & Asians have delayed growth compared to Africans and Hispanics, which means that Europeans and Asians undergo bone fusion later (usually 16) compared to as early as 14 in Africans and Hispanics.
If you are considering running a stack make sure that you can commit to running it for at least 6 months, ideally more than a year.
Stacks
NBA Stack
For maximum height gains, the most expensive and riskiest
IGF-1 LR330 - 50 mcg/every other day, subQ, preferably before bedHGH(Between 0.2 to 0.3 mcg) x bodyweight (kg) = weekly dosage/ 7 = daily dose, inject before bed SubQAIExemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.PTHHeightmaxing dosage is unknown, though it is clinically used between 25 mcg - 100 mcg everyday, I would recommend going no more than 25 mcg every other day. Inject subQ with IGF-1, before bed.
While I recommend PTH for people wishing to significantly increase height, its use will require monitoring of blood Vitamin D, Phosphorus and Calcium levels during its use and possible supplementation.Calcitriol0.25- 0.50 mcg/ day, take caution if using with PTH. Watch out for hypercalcemia.Optional Testosterone: any ester will be fine, though I recommend using Testosterone Propionate or Testosterone Enanthate. For height maxing a high dose of testosterone is not required, although those wishing to influence greater dimorphism may wish to increase the dosage. Do your own research if you plan to use Test.Run the stack for 4 weeks, take two weeks off, take 0.2mcg/kg HGH daily during off weeks. After 6 months: 4 weeks on, 6 weeks off, 0.2mcg HGH/day (this advice does not factor Test into account).Midstack
An affordable stack, best for most people, mild risk
IGF-1 LR350 - 80 mcg/ every other day, subQ, preferably before bedVitamin D3 (MK-7) 50K IU/ 3 times per week + 2.25mg K2/ with every D3 dose[1000 IU D3: 50mcg K2], I also recommend supplementing with magnesium, watch out for hypercalcemia.AIExemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.Poorcel
Questionable results on a budget
MK677 35 - 45 mg/day (bedtime) for 4 weeks, then every other day for two weeks at 20mg; repeat. I would also recommend mega dosing P-5-P throughout your cycle to decrease prolactin, especially if you are feeling symptoms of increased prolactin (gyno, decreased libido/mood, etc). For every 4 months on take 1 month off.AI (optional)Exemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.Stack Advise and Warnings
For those whose epiphyseal plates are closed and you want to increase your frame, you do not need to run these stacks with the same dosage.If you are older than 24 do not run any of these stacks (it's already over), as you will probably suffer from Acromegaly.Users on looksmax also recommend running compounds like mod GRF, hexarelin, CJC, etc. These compounds are all GH secretagogues, meaning they tell your brain to produce more GH, and as we already know administration of IGF-1 analogues like LR3 are far more effective. For this reason I think secretagogues are subpar to IGF/GH and should be avoided (unless you have no choice).There is still lots of debate around whether exogenous administration of growth factors causes certain cancers, some studies have shown for there to be a correlation, while others have disproved it. Do this at your own risk.“Our results do not generally support a carcinogenic effect of r-hGH, but the unexplained trend in cancer mortality risk in relation to GH dose in patients with previous cancer, and the indication of possible effects on bone cancer, bladder cancer and Hodgkin lymphoma risks, need further investigation.”
Elevated levels of GH/IGF-1 have also been reported to have side effects, most notably swelling of the feet or hands. If this occurs, discontinue use for a few weeks and try again at a lower dosage.Prior to injecting or taking anything make sure to do your own research on the side effects. Decrease the dosages according to how you feel, everyone tolerates drugs differently.Long term administration of GH/ IGF-1 has also been found to decrease insulin sensitivity, if you have diabetes or a family history reconsider heightmaxing. Exercise caution after the 4-6 month mark of running a stack, consider taking more time off and monitor your blood sugar.Stretching exercises/ hanging are also a cope, there is no evidence of any long term height increases.Lifestyle Changes
Some lifestyle changes that may contribute to increasing height:
- Eat a high protein diet (ideally >50% daily cal from protein)
- Ensure you get enough nutrients (use https://cronometer.com/), use supplements if you need to, make sure they are bioavailable.
- Eat in a slight surplus, 400 - 600 cal (unless you are obese, lose the weight first and then eat in surplus)
- Incorporate resistance training. For those serious about heightmaxing I would avoid exercises that compress your spine or pose a risk of damaging your joints (squats, deadlifts, OHP), instead opting for callisthenics and sprinting.
- Bone morphogenetic protein 3 was found to be elevated in fractured tissue (this may include microfractures). BMP3 is an agonist to other BMP’s, which means that more BMP3 = less bone growth (this doesn't mean you shouldn't exercise).
- Diet high in dairy products and calcium
- Sleeping >8 hours/ night consistently
- Some herbal supplements like Tongat Ali, Ashwagnada, etc may be useful for lowering oestrogen/ increasing testosterone; promoting sexual dimorphism.
- Depending on your situation you may also opt for using herbal supplements to control your oestrogen (delay fusion) and increase GH. The efficacy of these herbs are usually very questionable, and almost all (>90% of online vendors underdose their products).
- Decrease consumption of sugars (fructose, glucose, etc)
Conclusion
While this guide is far from perfect, hopefully I covered enough to help some of you on your heightmaxing journey. Best of luck and thanks for reading.
All this information was revealed to me in a dream
Inb4 greycel
Brodie said "your thread aint better than mine, but good job lil bro."Great thread but doesn't beat the current one in BOTB. You'll get a lot of redirects though from that thread.

Where tf can you even get DHT?Do you have any dht sources? I have testoserone and aromasin sources if you want to trade, my sources are legit and trusted not that testoserone from some untrusted company or that random aromasin with random russian writing
Look into ways you can make itWhere tf can you even get DHT?
I know there’s ways with proviron it’s just a hassle and a DHT gel would be 10X easier and time efficientLook into ways you can make it
They could be selling it in your country check for domestic or ask for a bodybuilder in your gym for a sourceI know there’s ways with proviron it’s just a hassle and a DHT gel would be 10X easier and time efficient
It’s ok. They most likely won’t give you direct height increases but are good building blocks for overall bone health.bro wtf everyone is arguing about the effects of these chemicals i aint puttin none of this shit in my body man too risky is it ok if i just take vit k and d2 supplements do HIIT training everyday and calisthenics and eat on a surplus with high protein and calcium diet and expose myself to 20 mins of sunlight everyday? and also is stretching cope? i will stretch anyway tho to increase flexibility ( im a pubertycel)
I like that you mentioned PTH but its totally impossible to source.
Introduction
As many of you know ‘heightmaxing’ is a popular topic of discussion on this website, which is no surprise given the importance of height on attractiveness as well as a plethora of other benefits associated with being taller.
I’m sure we’re all familiar with the importance of height, but there is a concerning deficit of information regarding methods and knowledge on how to engender an increase of height.
This shouldn’t come as much of a surprise, since the mechanisms behind increasing your height are very complex and we still don’t know a lot about the subject. Many factors work together to determine height and there is a lot of disagreement in the scientific community on the subject.
The purpose of this guide is to take a relatively simplistic, scientific and easy to understand approach to height maxing, which will hopefully dispel some of the confusion on the subject. The ‘science’ bits will be written in red for those wanting elaboration.
View attachment 2423234
Overview of the mechanisms involved in growing taller
1) Activation Phase: This is the beginning of bone growth. Cells called chondrocytes (cartilage) come together and proliferate (replicate). They create a blueprint made of cartilage, like a model for the bone to follow.
2) Osteoclast Recruitment and Resorption Phase (Hypertrophy Phase): Chondrocytes grow bigger (hypertrophy) and start turning the cartilage into hard stuff. Think of them as builders laying down the foundation for the bone.
3) Reversal Phase (Osteoblast Phase): A group of cells called osteoblasts moves in. They see the blueprint created by the cartilage and start adding bone on stop.
4) Formation Phase (Calcification Phase): The material the osteoblasts add becomes hard and strong because it calcifies, which is like turning it into concrete. Picture the bone getting denser and stronger.
5) Mineralization Phase (Ossification Phase): This is when the bone really takes shape. More bone cells come in, and they keep building and strengthening the bone, kind of like construction workers finishing a house.
6) Closure Phase (Epiphyseal Plate Closure): During adolescence, special plates at the ends of your long bones, called epiphyseal plates or growth plates, are active and contribute to your height. But once you reach a certain age, usually 15- 17, these plates close up.
View attachment 2423236
During osteoclastogenesis phases 1- 5 are constantly repeating in a loop until the closure phase.
The phase in osteoclastogenesis (bone growth) which contributes to enlarging your longitudinal height the most is the activation phase, which starts when you are an embryo and ends with the closure phase.
Now the question becomes: how do I enhance the mechanisms of the activation phase.
During the activation phase cartilage grows through proliferation and differentiation.
Cell proliferation = Cell gets bigger + Cell divides, AKA More cells
View attachment 2423237
For the purpose of heightmaxing, proliferation is one of the important mechanisms that drives height growth.There are some things we can do to increase the proliferation and hypertrophy of cartilage in the growth plate. This is done through bone growth factors, which work through a variety of different mechanisms and pathways.
We need to do everything possible to enhance cell proliferation and cell size in the growth plate.
What we need to do to heightmax
1) Increase cartilage proliferation (replication)
2) Increase cartilage hypertrophy (size)
3) Delay the closure phase
One of the ways we can increase proliferation and hypertrophy is with growth factors (a subset of cytokines).
An Introduction To Growth Factors & Hormones
Known bone growth factors (outside of foetal development) include:
- Insulin-like growth factor-1 (IGF-1) is the most abundant growth factor deposited in the bone matrix and stimulates cell proliferation and function, and survival of osteoblasts.
- There are several reports demonstrating the synergistic effects of IGF-1 and PTH on bone remodelling and establishing the involvement of locally produced IGF-1 in the anabolic effects of PTH
- PTH can exert both catabolic and anabolic effects on bone. It is well established that daily injections of low doses of PTH increase bone mass in animals and humans
- Transforming growth factor beta (TGF-β)
- TGF-β1
- TGF-β3
- Sort of a double edged sword, can cause an increase of bone mass but also osteoporosis, it is best to use this as little as possible.
- Fibroblast growth factors (FGF)
- FGF 1 - 10
- FGF18
- Endogenous FGF-2 was found to be necessary for the bone anabolic effects of PTH and BMP-2 in mice
- Platetet- Derived Growth Factor (PDGF)
- Growth Differentiation Factor (GDF)
- GDF3
- GDF6
- GDF10
- Fibroblast Growth Factor (FGF)
Hormones also play a role in height and morphology, a brief overview of which is provided below:
- Growth Hormone:
- Stimulates IGF-1 growth factor AND IGF-1 receptor production. Growth hormone (GH) is a peptide hormone secreted from the pituitary gland under the control of the hypothalamus. It has been reported that both GH-deficient humans and mice have reduced longitudinal bone growth
- Testosterone & DHT:
- Broadens Shoulders & promotes sexual dimorphism. Androgens can also modulate growth plate maturation and closure, and thus affect longitudinal bone growth. In addition, androgens regulate trabecular and cortical bone mass, and inhibit bone loss
- Oestrogen (Estrogen):
- Causes the hips to widen and become rounded & speed up the rate of Growth Plate fusion (more on this in part 4). Oestrogen is also needed for healthy bones.
- Thyroid Hormones: Thyroid hormones, particularly thyroxine (T4) and triiodothyronine (T3) promote chondrocyte proliferation and the synthesis of collagen and other bone matrix proteins.
Something rarely mentioned in heightmaxing is Growth Factor receptors, growth factor receptors and growth factors as two puzzle pieces, they need each other to work.
There aren’t many ways to directly increase Growth factor receptors, but some studies suggest that increasing one growth factor can signal others to proliferate.
What this also means is that depending on your specific distribution of growth factor receptors your growth will be somewhat random. People who have more receptors in their legs/ epiphyseal plate will experience more growth in that area than someone with more receptors in their shoulders or nose.
View attachment 2423238
Primary Growth Factors - Factors that lead to the most growth
An overview of some of the process' involved promoting bone growth
Applying Growth Factors
IGF-1 (IGF-1 LR3)
One of the most popular growth factors on looksmax for heightmaxing is IGF-1, which granted its price and efficacy should come as no surprise . Another advantage of IGF-1 is that it binds and activates its own receptor.Among the insulin-like growth factor 1 (IGF-1) analogues, the one with the best balance between potency and half life is IGF-1 LR3. It has a half life of between 20-30 hours and a stronger binding affinity than naturally occurring IGF-1
Growth Hormone (HGH)
Again, a very popular growth factor on this website. Growth hormone (GH) is a peptide hormone secreted from the pituitary gland under the control of the hypothalamus. GH, along with its binding protein (GHBP), regulates growth directly through the GH receptor (GHR) and indirectly by stimulating liver and skeletal IGF-1 expression.It has been reported that GH stimulates osteoblast proliferation and collagen production either directly and/or indirectly by increasing IGF-1 and IGF binding protein (IGFBP) productionThese effects make GH useful, mostly due to its signalling properties and ability to upregulate the number of Growth Hormone receptors. While the increase in IGF-1 is also useful, we already know that synthetic IGF-1 analogues like IGF-1 LR3 are more potent, meaning that both GH and IGF-1 LR3 could be used synergistically. PTH
A compound not typically discussed on this forum is Parathyroid hormone.Parathyroid hormone (PTH), also called parathormone or parathyrin, is a peptide hormone secreted by the parathyroid glands.As mentioned earlier, PTH and IGF-1 are known to have synergistic effects, therefore it is advantageous to be running both IGF and PTH in the same stack.
View attachment 2423240
Osteogenic differentiation of BMSCs treated with vehicle (-), IGF-1 (50 ng·mL-1), PTH (100 nmol·L-1), or both as assessed by alkaline phosphatase.
We can see that using both IGF and PTF gives us significantly more growth.
Secondary Growth Factors - Factors That Support Growth
Calcitriol
Calcitriol is the biologically active form of vitamin D in the body. It is also known as 1,25-dihydroxyvitamin D3 or simply activated vitamin D. It is up to 1,000 times more potent than vitamin d2 and d3, making it ideal for supporting growth.
Testosterone & DHT
By far one of the most influential androgens on height and the development of a sexually dimorphic skeleton. The androgen mechanism of action on height is not well understood, but it is known to stimulate longitudinal bone growth as well as radial bone growth, thereby increasing the cortical bone size.
Lifestyle/ Diet
By far one of the most under looked growth factors is your lifestyle, it is often the easiest and one of the most impactful on your height.Eating enough food is vital to create the building blocks of hormones/ growth factors, ultimately increasing your height. It has been suggested that in addition to adequate intake of macro and micronutrients (vitamins, minerals, amino acids) intermittent fasting can also be beneficial for raising IGF-1 and increasing insulin sensitivity. Diets high in protein and dairy (not including cheese) were also found to elevate IGF-1.Adequate sleep, minimal stress and regular exercise are also seen to have positive effects on height.Delaying Growth Plate Fusion“Oestrogen causes maturation of the growth plate, accelerating skeletal maturation and the accumulation of minerals into the cartilage. Oestrogen also promotes the closure of the physis, stopping the axial growth of the bone. Decreases in total oestrogen or oestrogen receptor sensitivity results in longer bones and tall stature”What this means is that oestrogen is one of the driving forces behind signalling the closure phase. One of the ways Oestrogen can be regulated is via a class of drugs called antioestrogens.
Antioestrogens I recommend:
- Exemestane (Aromasin) is relatively easy to get, has a long half life (24 hours), low side effects and decent bioavailability.
- Letrozole has also been shown to delay the fusing of the growth plates in mice. When used in combination with growth hormone, letrozole has been shown effective in one adolescent boy with a short stature. Mice administered with Letrozole were also found to have higher testosterone levels. I recomend cycling Lerozole with Aromasin.
Growing Taller
If you are 15 and over I recommend getting an x- ray done of your epiphyseal plate to confirm whether or not it has fused. Complete fusion of the growth plate most commonly occurs between 15-17 in males (and no, you’re probably not an exception).
If your epiphyseal plate is open great, if not then you can still apply some of these methods to improve your frame. All bones fuse at different times, so even though your epiphyseal plate is sealed your other bones, such as the tibia and collarbone may still be open, allowing you to grow (more on this below).
It is also worth noting that Europeans & Asians have delayed growth compared to Africans and Hispanics, which means that Europeans and Asians undergo bone fusion later (usually 16) compared to as early as 14 in Africans and Hispanics.
If you are considering running a stack make sure that you can commit to running it for at least 6 months, ideally more than a year.
Stacks
NBA Stack
For maximum height gains, the most expensive and riskiest
IGF-1 LR330 - 50 mcg/every other day, subQ, preferably before bedHGH(Between 0.2 to 0.3 mcg) x bodyweight (kg) = weekly dosage/ 7 = daily dose, inject before bed SubQAIExemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.PTHHeightmaxing dosage is unknown, though it is clinically used between 25 mcg - 100 mcg everyday, I would recommend going no more than 25 mcg every other day. Inject subQ with IGF-1, before bed.
While I recommend PTH for people wishing to significantly increase height, its use will require monitoring of blood Vitamin D, Phosphorus and Calcium levels during its use and possible supplementation.Calcitriol0.25- 0.50 mcg/ day, take caution if using with PTH. Watch out for hypercalcemia.Optional Testosterone: any ester will be fine, though I recommend using Testosterone Propionate or Testosterone Enanthate. For height maxing a high dose of testosterone is not required, although those wishing to influence greater dimorphism may wish to increase the dosage. Do your own research if you plan to use Test.Run the stack for 4 weeks, take two weeks off, take 0.2mcg/kg HGH daily during off weeks. After 6 months: 4 weeks on, 6 weeks off, 0.2mcg HGH/day (this advice does not factor Test into account).Midstack
An affordable stack, best for most people, mild risk
IGF-1 LR350 - 80 mcg/ every other day, subQ, preferably before bedVitamin D3 (MK-7) 50K IU/ 3 times per week + 2.25mg K2/ with every D3 dose[1000 IU D3: 50mcg K2], I also recommend supplementing with magnesium, watch out for hypercalcemia.AIExemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.Poorcel
Questionable results on a budget
MK677 35 - 45 mg/day (bedtime) for 4 weeks, then every other day for two weeks at 20mg; repeat. I would also recommend mega dosing P-5-P throughout your cycle to decrease prolactin, especially if you are feeling symptoms of increased prolactin (gyno, decreased libido/mood, etc). For every 4 months on take 1 month off.AI (optional)Exemestane (Aromasin) 25mg/every other day or Letrozole every 4 days at 2.5mg. Depending on how long you plan to run a stack for, I would consider cycling this after more than 4-5 months.Stack Advise and Warnings
For those whose epiphyseal plates are closed and you want to increase your frame, you do not need to run these stacks with the same dosage.If you are older than 24 do not run any of these stacks (it's already over), as you will probably suffer from Acromegaly.Users on looksmax also recommend running compounds like mod GRF, hexarelin, CJC, etc. These compounds are all GH secretagogues, meaning they tell your brain to produce more GH, and as we already know administration of IGF-1 analogues like LR3 are far more effective. For this reason I think secretagogues are subpar to IGF/GH and should be avoided (unless you have no choice).There is still lots of debate around whether exogenous administration of growth factors causes certain cancers, some studies have shown for there to be a correlation, while others have disproved it. Do this at your own risk.“Our results do not generally support a carcinogenic effect of r-hGH, but the unexplained trend in cancer mortality risk in relation to GH dose in patients with previous cancer, and the indication of possible effects on bone cancer, bladder cancer and Hodgkin lymphoma risks, need further investigation.”
Elevated levels of GH/IGF-1 have also been reported to have side effects, most notably swelling of the feet or hands. If this occurs, discontinue use for a few weeks and try again at a lower dosage.Prior to injecting or taking anything make sure to do your own research on the side effects. Decrease the dosages according to how you feel, everyone tolerates drugs differently.Long term administration of GH/ IGF-1 has also been found to decrease insulin sensitivity, if you have diabetes or a family history reconsider heightmaxing. Exercise caution after the 4-6 month mark of running a stack, consider taking more time off and monitor your blood sugar.Stretching exercises/ hanging are also a cope, there is no evidence of any long term height increases.Lifestyle Changes
Some lifestyle changes that may contribute to increasing height:
- Eat a high protein diet (ideally >50% daily cal from protein)
- Ensure you get enough nutrients (use https://cronometer.com/), use supplements if you need to, make sure they are bioavailable.
- Eat in a slight surplus, 400 - 600 cal (unless you are obese, lose the weight first and then eat in surplus)
- Incorporate resistance training. For those serious about heightmaxing I would avoid exercises that compress your spine or pose a risk of damaging your joints (squats, deadlifts, OHP), instead opting for callisthenics and sprinting.
- Bone morphogenetic protein 3 was found to be elevated in fractured tissue (this may include microfractures). BMP3 is an agonist to other BMP’s, which means that more BMP3 = less bone growth (this doesn't mean you shouldn't exercise).
- Diet high in dairy products and calcium
- Sleeping >8 hours/ night consistently
- Some herbal supplements like Tongat Ali, Ashwagnada, etc may be useful for lowering oestrogen/ increasing testosterone; promoting sexual dimorphism.
- Depending on your situation you may also opt for using herbal supplements to control your oestrogen (delay fusion) and increase GH. The efficacy of these herbs are usually very questionable, and almost all (>90% of online vendors underdose their products).
- Decrease consumption of sugars (fructose, glucose, etc)
Conclusion
While this guide is far from perfect, hopefully I covered enough to help some of you on your heightmaxing journey. Best of luck and thanks for reading.
All this information was revealed to me in a dream
Inb4 greycel
I'm being honest though. If it was better, I'd be glad to remove my thread since I want people to get taller. No ego or pride involved.Brodie said "your thread aint better than mine, but good job lil bro."
Just funny that's allI'm being honest though. If it was better, I'd be glad to remove my thread since I want people to get taller. No ego or pride involved.

BasedHgh and ghrp are to increase hgh, igf1 is what hgh turns into to proliferate growth plate cartilage. And igf1 lr3 is a more potent form of igf1. It stays in the bloodstream way longer and doesn’t bind to igf binding proteins like normal igf1 would. Also I’m most likely going to be applying mechanical stres on my bones also because of Wolffs law at the same time, I’m 5”9 my dad is 5”11 and I want to grow to atleast 6”3-6. And also since I’m going to take testosterone/dht I’ll 100% have a bigger coc, wider clavicles, etc